Published January 2026 by St. Martin’s Press
Thank you, NetGalley and publisher, for sending this book for review consideration.
Why would a medical doctor write about ways to die? Aren’t they supposed to keep people alive?
Yes, and that’s why Dr. Ashely Alker, a “death escapologist”, wrote 99 Ways to Die. As an emergency medicine specialist, she says this book is bad for business. Reading it, and following her advice, may keep you out of her emergency room. Better yet, it may save your life.
Dr. Adler briefly shares her pre-medical life and education, including overseas study for a master’s degree in public health. She relates personal experiences with illness and the healthcare system, which led her to medical school and residency.
The table of contents reads like a textbook of emergency medicine, in that it includes both illnesses and situations that can lead to illness. Some of them you have no doubt heard of.
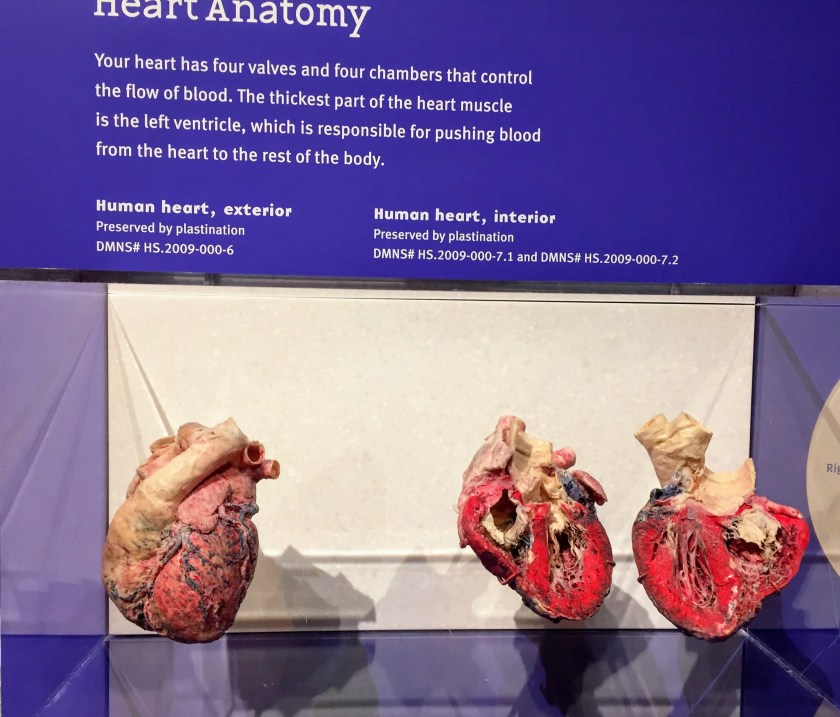
- Heart Attacks
- Cancer
- Ebola virus
- Nuclear blast radiation
But have you heard of
- Schistosomiasis,
- Mad Cow disease,
- Venomous agent X,
- Takotsubo cardiomyopathy
And you’ve heard of but may not believe can be deadly.
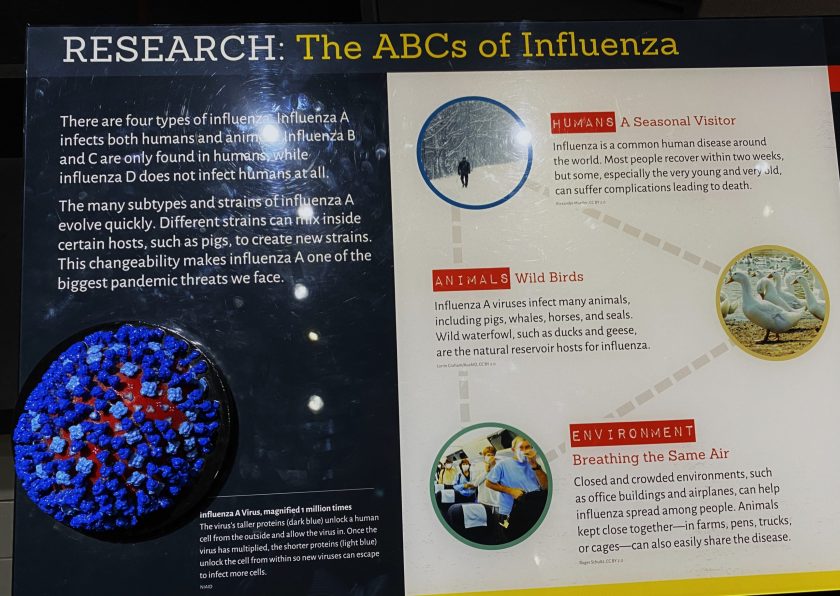
- Influenza,
- Measles,
- High Blood Pressure,
- Pregnancy,
- Health Influencers (yes, she really wrote this)
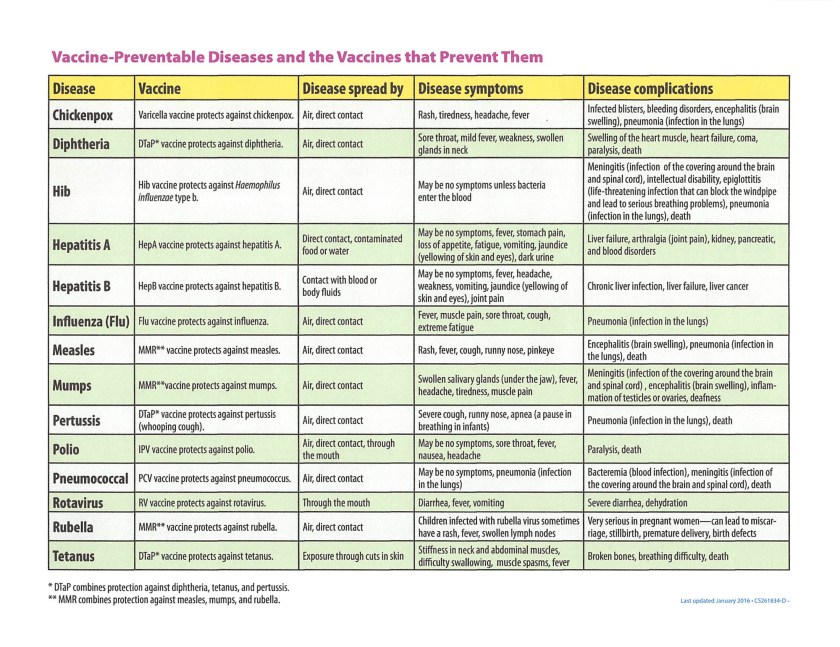
She devotes ample discussion to infections, both bacteria, viral, fungi, and even parasites. One whole chapter is on vaccine-preventable infections (obviously, she advocates vaccination)
One of the top five frequent causes of death is accidental trauma, which is often overlooked in discussions of preventive medicine. Not Dr. Adler. She details the ways things like drugs, animals, vehicle crashes, crime, sports, weather, and war can harm and kill us. And don’t forget the dangers of food and water!
You may be thinking this book must be highly technical. She does use scientific names and terms, which she explains in simple language. Her tone is engaging and conversational. She is blunt, sometimes humorous, but always perfectly serious.
She shares stories of her own patients with these conditions; details changed for privacy. Is some of it gory or scary? Maybe, depending on your comfort level and how much you want to know about the human body and how it can be misused and abused.
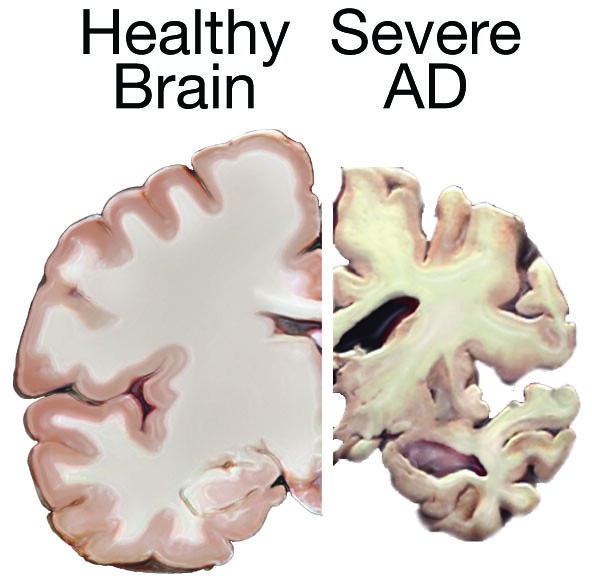
Disease and death affect all of life and history, as she points out in discussing the impact of the influenza epidemic of 1918 and the COVID-19 pandemic of 2020. I found her discussion of the atomic bombs dropped on Hiroshima and Nagasaki, Japan in World War II particularly poignant.
The initial blasts killed over 200,000 civilians, with many more dying later from radiation illness. In her review of biological and chemical warfare, she suggests we consider carefully who we put into power.
From this book, you will learn that health is more than knowing your blood pressure and cholesterol. Our risk of disease is more due to where and how we live, and our socioeconomic status. The most important number for your health may be your zip code in the United States.
None of us expect to die from an automobile collision, hypothermia, homicide, drowning, tornado, poisoning, insect bite, or war, but we might and she explains how to avoid it. Common sense things-wear a seat belt, dress for the weather, apply insect repellent, don’t believe medical misinformation you read online. Learn CPR and save someone else’s life.
I’m a physician and worked in ERs, but I still learned from her book. So, I believe you will also. Her main takeaway is to value and care for your body, you only have one. As she wrote in her dedication
May we all be alive this time next year.
Dr. Ashely Alker
Read an excerpt
Note: She does not intend this book to replace advice from your own personal physician. References to CDC recommendations are to those issued before January 1, 2025.
The Author
Ashely Alker, M.D., M.Sc., is an emergency medicine physician on a mission to improve public health. While completing her master’s degree, Dr. Alker studied at Harvard School of Public Health’s multinational institute in Cyprus. She lived near the United Nations Green Zone and worked in humanitarian affairs at the Unit for the Rehabilitation of Victims of Torture.

After graduating from the George Washington University School of Medicine, Dr. Alker served as a healthcare advisor for a member of the US Congress. During her residency in emergency medicine at the University of California, San Diego, Dr. Alker became a technical consultant and medical screenwriter, improving medical accuracy on over twenty shows, including TV and film for Netflix, Hulu, HBO, and Disney.
Her nonprofit, Meaningful Media, connects writers, artists, and reporters with certified public health experts to develop scientifically accurate messaging.
Images in this Post
The book image and Dr. Alker’s photo are from her website.
What do you think?
What do you think about a physician writing a book about dying?
What is the most unusual, bizarre, or unexpected cause of death that you know about?
How will reading this review and/or the book impact your idea of what will cause your own death?
Exploring the HEART of Health
I’d love for you to follow this blog. I share information and inspiration to help you transform challenges into opportunities for learning and growth.
Add your name to the subscribe box to be notified of new posts by email. Click the link to read the post and browse other content. It’s that simple. No spam.
I enjoy seeing who is new to Watercress Words. When you subscribe, I will visit your blog or website. Thanks and see you next time.
Use this search box for related posts on this blog or other topics of interest to you.
Dr. Aletha
- About Dr. Aletha
- How to Use this Site
- Make Your Life Easier
- Search by Category
- Share the HEART of health
- my Reader Rewards Club
- RoboForm Password Manager