This information is current as of the date of original publication or update but may have changed by the time you read this. Do not use this information for diagnosis or treatment purposes. Before making health decisions, discuss with a qualified healthcare professional.
One way physicians help people stay healthy is by offering screening tests. These tests can detect conditions for which prevention or treatment increase life span, prevents disability, and promotes wellness.
Screening tests are for people without symptoms of the condition in question. Recommendations for screening are usually based on patient-specific factors such as gender, age, family history, health habits, and other medical issues.
Screening tests recommended by medical organizations or governmental health agencies are usually covered by insurance without a copay.
Screening tests can be inconvenient and uncomfortable. They may create anxiety if further testing is needed to confirm results. These expenses may not be covered by insurance.
Most of the time, screening tests find no disease.
As we get older and remain healthy, it is reasonable to question whether screening tests are necessary or even helpful. Might it actually be harmful to screen older adults for conditions they likely never will develop, or if they do, will not cause premature death?
Doctors and patients are asking that question more often. This article from KFF Health News explores those questions.
3 Medical Routines That Older People May Not Need
By Paula Span, May 22, 2026
Enough time had passed since the patient’s previous colonoscopy that she met the criteria to undergo another, said Steven Itzkowitz, a gastroenterologist at the Icahn School of Medicine at Mount Sinai in New York.
She was in “reasonably good health,” and the risks of the procedure — bleeding, reaction to anesthesia, perforation of her colon — were fairly low. But she was 85. And she would need to briefly discontinue the blood thinners she took because of the cardiac stents keeping her arteries open; doing so could increase the risks.
Had Itzkowitz and his patient faced this decision five years ago, he might have scheduled the screening “without even thinking about it,” he said. But recent research has shown again that the benefits of a repeat colonoscopy are slim after age 75.
Now, he said, “I’m saying to myself, ‘What are we accomplishing here?’”
He’s not the only doctor — or patient — having second thoughts. The risks and benefits of common screenings, procedures, and drugs add up differently at advanced ages, and research continues to point out fresh examples of some that may become unnecessary.
Recently, investigators have taken on questions about common skin lesions that probably don’t need to be removed, a widely used thyroid medication that many older patients can safely discontinue, and colonoscopies that reduce colon cancer mortality so slightly that the risks may outweigh the benefits.
Ugly but Probably Harmless-Actinic Keratosis
The reddened or rough patches on the skin are called, in doctor-speak, actinic keratoses. Because they result from long-term sun exposure, they usually appear on faces, scalps, forearms, and the backs of hands.
Such lesions appear most commonly on older patients. One large study of traditional Medicare beneficiaries found that over a five-year period, almost 30% were diagnosed with an actinic keratosis. Then what?
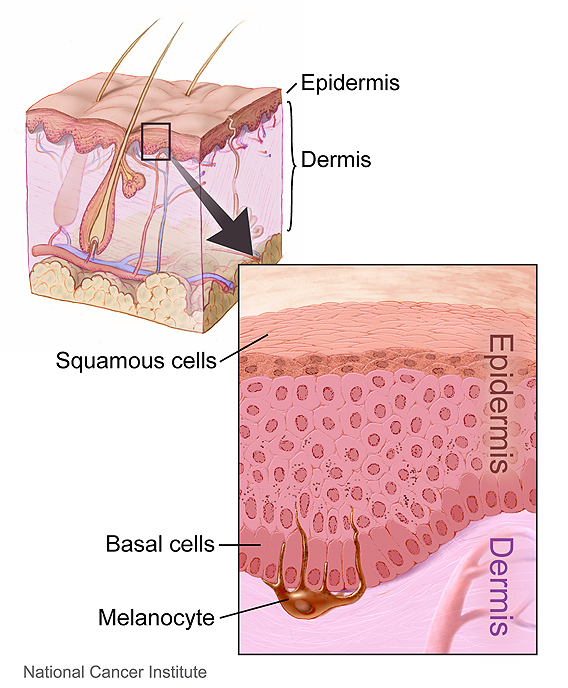
Source: National Cancer Institute
Creator: Don Bliss (Illustrator)
This image is in the public domain and can be freely reused. Please credit the source and, where possible, the creator listed above.
“The vast majority of the time, they’re removed,” said Allison Billi, a dermatologist at the University of Michigan and an author of a recent commentary on the topic in JAMA Internal Medicine. That typically involves cryosurgery (freezing with liquid nitrogen), topical creams, or laser therapy.
The rationale: The patches could become cancerous. But “for the average patient with no history of skin cancer, there is less than a 1-in-1,000 chance of it progressing to skin cancer,” Billi said, citing a 2013 meta-analysis. The lesions are far more likely to disappear on their own.
“The treatment may be more burdensome than the condition itself,” she added. Removal “is actually extremely painful, both during and after.” It can cause swelling, irritation, and lasting discoloration.
Besides, an actinic keratosis will probably reappear, or new ones will emerge. “This is a chronic condition,” Billi said.
She has proposed active surveillance, instead: Primary care doctors could observe the lesions annually for warning signs like bleeding, pain, or rapid growth, which might warrant removal. But “in many cases, it’s not necessary,” she said.
She does recommend using sunscreen, however. (affiliate)
“We don’t always need to do everything we can do.”
Dr. Allison Billi, dermatologist
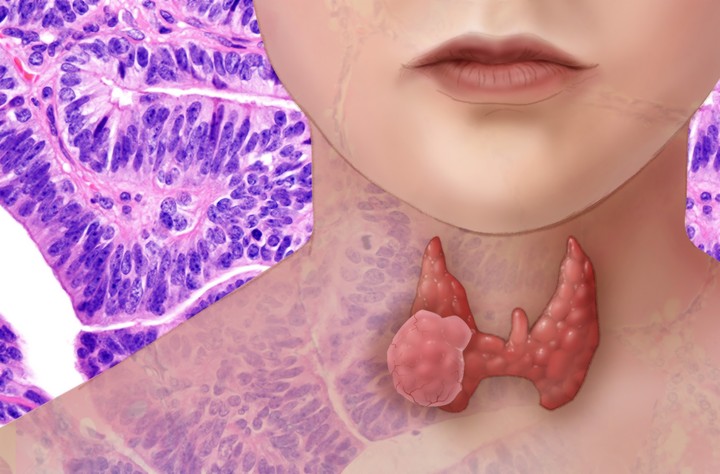
Questionable Treatment-Hypothyroidism
Patients take levothyroxine, one of the world’s most frequently prescribed drugs, when their thyroid glands can’t produce sufficient thyroid hormone.
With this condition, called hypothyroidism, “people gain weight. They have less energy. Their hair and skin are dry,” explained Jacobijn Gussekloo, a primary care doctor and researcher at Leiden University Medical Center in the Netherlands. “Everything slows down.”
Doctors also increasingly prescribe it for a borderline condition called subclinical hypothyroidism, which usually causes no symptoms but can progress to hypothyroidism.
Most patients take the drug for life — but do they have to? Gussekloo’s team has found that in many older adults with subclinical hypothyroidism, hormone levels normalize on their own.
The researchers have also reported that among older people with the condition, levothyroxine had no effect on symptoms and “no apparent benefit.”
Like any drug, it can also cause harm. It may interact with other medications that older patients typically take. Moreover, “it requires frequent lab tests and follow-ups, more visits and expense,” said Maria Papaleontiou, an endocrinologist at the University of Michigan and an author of an editorial in JAMA accompanying the latest Dutch study.
“In high doses, it can cause hyperthyroidism, which can lead to cardiac arrhythmias and bone loss,” she added. Patients taking it also have to adjust their diets and meal schedules.
To determine whether some patients could stop taking levothyroxine, the Dutch researchers devised a protocol that gradually reduced doses over 30 weeks, with ongoing lab testing and consultations with doctors.
After a year, a quarter of the 370 participants, all over 60, had discontinued the drug while maintaining healthy thyroid function. Most had been on lower doses to begin with.
Patients shouldn’t stop levothyroxine on their own, Papaleontiou cautioned. Discontinuation requires tapering off gradually, with testing and monitoring. Some patients will always need the drug.
But it appears that “a select group of adults over 60 may not require this treatment lifelong,” Papaleontiou said.
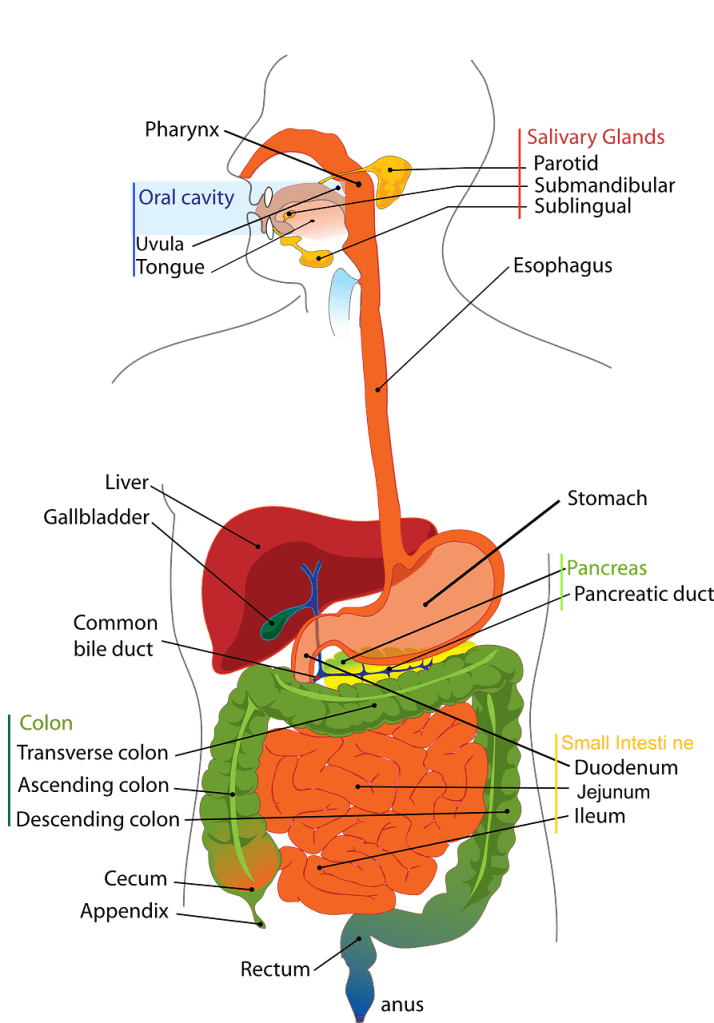
A Screening With Risks-Colonoscopy
The question of when older patients can safely stop screening for colon cancer has prompted years of debate. The influential U.S. Preventive Services Task Force gives the screening a lukewarm C rating after age 76, calling the benefit “small.”
Yet almost 60% of older patients who have had previous colonoscopies and face limited life expectancies (less than five years) are advised to undergo another screening, a 2023 study found.
As a gastroenterologist at the University of California-San Diego, Samir Gupta regularly encounters this issue with older patients. “I know they really have a low risk of colon cancer, and I’m putting them through more risk,” he said.
The risk of complications following a colonoscopy rise with age. One study found that nearly 7% of patients over 75 had a hospitalization or emergency room visit within a month of the procedure.
Is it worth it? Gupta is the lead author of a new study of almost 92,000 Veterans Affairs patients over 75 who had previous colonoscopies. In about 28%, the procedure had found an adenoma, a type of polyp that can become cancerous. Though only a small fraction do, gastroenterologists generally remove them.
The researchers found that after 10 years, veterans with a previous adenoma were more likely to develop colon cancer than those without one, though the rate was extremely low in both groups.
But just 0.5% — yes, one-half of 1% — of those with a previous adenoma died of colon cancer, compared with 0.4% of those without one. “A tiny difference,” Gupta said.
Both groups were dwarfed by the number of veterans — almost half — who died within the decade of other causes.
“Even if the procedure goes well, you’ll either find nothing or you’ll find something that’s not going to have real impact on your longevity,” said Itzkowitz, an author of an editorial published alongside the study.
Yet he has found that many patients who have had polyps removed want to continue colonoscopies.
It is hard to shift established medical norms. Efforts to “deprescribe” drugs can meet with opposition from both patients and health care professionals.
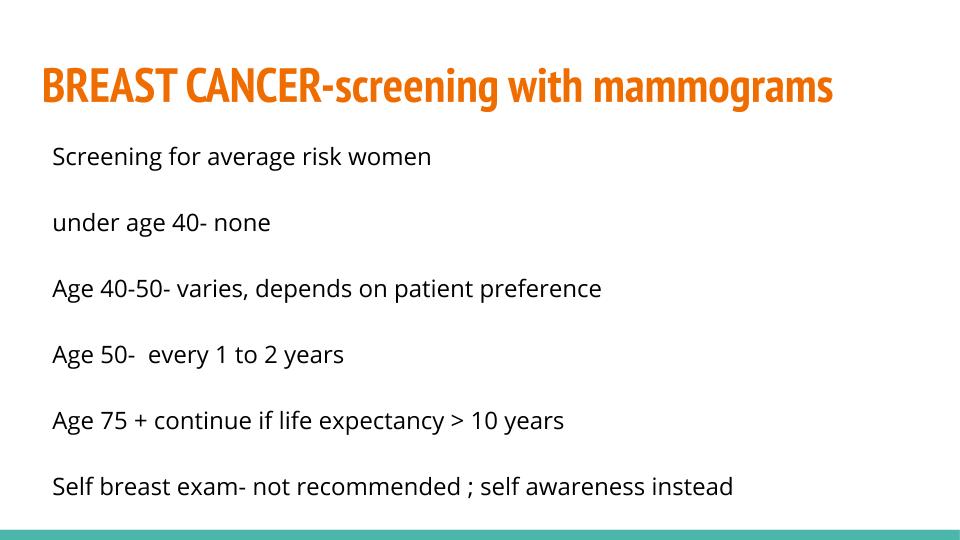
Many older women continue having mammograms past the point of documented benefit, and older men often undergo prostate cancer screening beyond the recommended age.
Colonoscopies are less pleasant, so perhaps older patients will be glad to forgo them. “Even with polyps, the chance of dying from colon cancer is so low compared to everything else that can get you,” Itzkowitz said.
So he told his 85-year-old patient that she could skip another colonoscopy. She seemed pleased.
The New Old Age is produced through a partnership with The New York Times.
KFF Health News is a national newsroom that produces in-depth journalism about health issues and is one of the core operating programs at KFF—an independent source of health policy research, polling, and journalism. Learn more about KFF.
This article first appeared on KFF Health News and is republished here under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
Images in this Post
The graphics were not in the original KFF article. The cover image was generated by AI in WordPress.
Exploring your health
Screening medical tests are not just for older people. Screening evaluations are recommended for people of all ages. all ages.
Do you know what screening tests are recommended for you? You can consult an online resource, but the best source is your own personal physician, who knows your past, current, and family medical history.
What does or would motivate you to have screening tests, or not?
What benefit, or not, have you received from screening tests?
Exploring the HEART of Health
I’d love for you to follow this blog and follow me on social media.
I share information and inspiration to help you transform challenges into opportunities for learning and growth.
Add your name to the subscribe box to be notified of new posts by email. Click the link to read the post and browse other content. It’s that simple. No spam.
I enjoy seeing who is new to Watercress Words. When you subscribe, I will visit your blog or website. Thanks and see you next time.
Dr. Aletha
- About Dr. Aletha
- How to Use this Site
- Make Your Life Easier
- Search by Category
- Share the HEART of health
- my Reader Rewards Club
- RoboForm Password Manager