
This post has been updated July 2025
Both doctors and patients have mixed emotions about tests done to screen for disease. We, as physicians, want to help patients stay healthy, prevent disease, and treat problems early and effectively.
However, the time spent explaining, ordering, performing, and reviewing these tests means less time available to manage patients’ existing medical problems.
I agree with Dr. William Zinn, a family physician in Boston, who wrote
“Keeping track of the ever-increasing health maintenance requirements and cancer screening sometimes make it hard to remember why the patient came to the office in the first place.”
JAMA, January 7, 2020
For patients the issues are similar. While they want to stay healthy, prevent disease, and get treated promptly, they don’t like the inconvenience, time away from work, cost, and sometimes discomfort the tests require.
What are screening tests?
A screening medical test is done to uncover a disease or disorder in a person who may or may not be at risk for it and who otherwise feels well and has a normal exam. Suppose we are considering screening a group of people for disease X. Let’s start by dividing them into 3 groups.
- Those with no symptoms, feel fine, at average risk of health condition X.
- Those with no symptoms, feel fine, at increased or high risk of condition X.
- Those who have symptoms suggestive of condition X, or have had other testing that suggests they might have it
Screening for X in groups 1 and 2 might be appropriate, based on medical guidelines, physician judgement, and patient preference. For group 3, with symptoms of condition X, testing would be considered diagnostic; a doctor would test for X, and possibly other conditions that the symptoms suggest.
Diagnostic vs Screening
That might seem like a picky difference, but there are several implications for both doctors and patients.
Documentation- The medical record must document accurately the reason a test is being ordered and done. This is necessary for billing because inaccurate coding can make doctors and clinics liable for fraud. Also, the government and other payers are starting to judge doctors’ quality of care based on medical record audits of care given or not given, and why.
Interpretation and Follow-up-A test is rarely interpreted in isolation. The history and exam together with the test determine if further testing or treatment is needed.
Reimbursement– Most if not all insurances, including Medicare, reimburse differently based on whether a test is diagnostic or screening. And this usually determines how much the patient pays for each. Screening tests are usually covered 100% while diagnostic testing may require a deductible or copay .
A Country Doctor Writes blog explains this dilemma in detail –
But because in the inscrutable wisdom of the Obama Affordable Care Act, it was decided that screening colonoscopies done on people with no symptoms whatsoever are a freebie, whereas colonoscopies done when patients have symptoms of colon cancer are subject to severe financial penalties.
HANS DUVEFELT, MD
This link at FamilyDoctor.org helps explain
Health Insurance: Understanding What It Covers
Cervical cancer screening frequency also now takes into account a woman’s HPV, human papilloma virus, status. Go here to learn
When should a woman begin cervical cancer screening, and how often should she be screened?
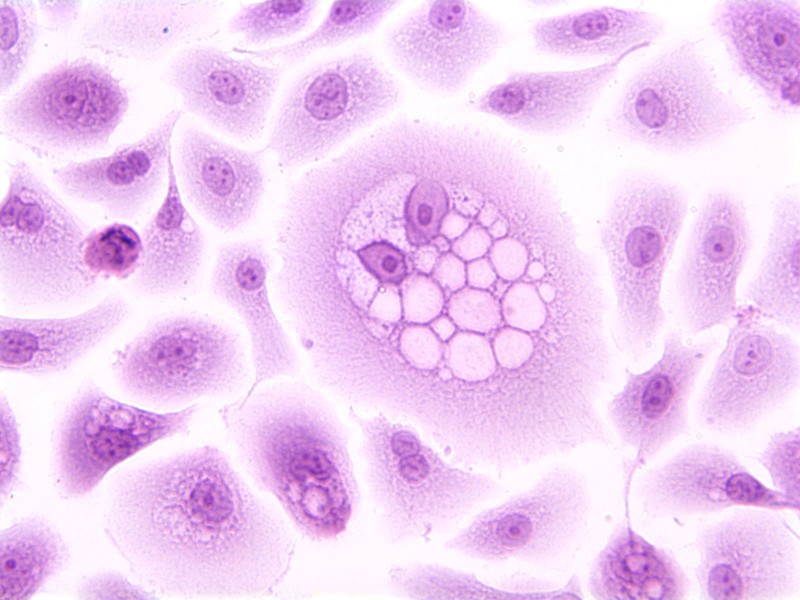
A koilocyte is a squamous epithelial cell that has undergone structural changes as a result of infection by human papillomavirus (HPV). This image of a koilocyte shows human ectocervical cells (HEC) expressing HPV-16 E5 oncoprotein, and immortalized with HPV-16 E6 and E7 oncoproteins. Formation of koilocytes requires cooperation between HPV E5 and E6 oncoproteins. The cell culture is stained with hematoxylin and eosin (H&E).National Cancer Institute \ Georgetown Lombardi Comprehensive Cancer Center, Ewa Krawczyk, public domain
Does disease screening make a difference?
Screening tests don’t prevent disease although they may be helpful for health maintenance or improvement. They may prevent progression or complications of a disease, but don’t prevent its onset.
They may not prevent death from the disease, although we like to believe they do. Screening may diagnose the disease before symptoms develop, so the patient lives longer with the disease, but not affect the eventual outcome.
Colon cancer is occurring at younger ages so the age to begin screening is now under age 50. Doctors can offer patients an option that is more accurate than the stool blood test and less invasive than colonoscopy.
Stool DNA testing looks for certain DNA or gene changes in cells that can get into the stool from polyps (pre-cancerous growths) or cancer cells. It may also check for blood in the stool.
For this test, people use an at-home kit to collect a stool sample and mail it to a lab. Cologuard® is the name of the stool DNA test that is currently FDA-approved. This stool test needs to be done every 3 years.
When should we offer screening tests?
If there is a clear benefit to patients from an effective treatment available to make a difference in the disease course or
If knowledge of the condition helps the patient and family make choices about managing the condition’s likely course or the need for family members to be screened
If the test is reliable enough to identify most people with the disease without falsely identifying people who don’t have it. The scientific terms for this are sensitivity and specificity.
When the benefits clearly outweigh the risks and costs.
How to decide on screening for yourself
These are just some of the factors involved in deciding when to undergo screening tests. To make an intelligent decision about your own screening, you need a physician who reviews your past and current medical history, your family history, and your health goals.
Then the doctor can make recommendations based on your needs and desires with the help of expert guidelines published by medical organizations that carefully review the medical literature.
Help your doctor help you by scheduling a health maintenance visit rather than bringing it up when you are there sick or for chronic care. These discussions deserve your physician’s full attention.
from the National Institutes of Health.
To Screen or Not to Screen
¿Hacer o no hacer pruebas de detección?
Exploring the HEART of health maintenance
I’d love for you to follow this blog. I share information and inspiration to help you transform challenges into opportunities for learning and growth.
Add your name to the subscribe box to be notified of new posts by email. Click the link to read the post and browse other content. It’s that simple. No spam.
I enjoy seeing who is new to Watercress Words. When you subscribe, I will visit your blog or website. Thanks and see you next time.
- About Dr. Aletha
- How to Use this Site
- Make Your Life Easier
- Search by Category
- Share the HEART of health
- my Reader Rewards Club
- RoboForm Password Manager
Dr. Aletha
RoboForm Password Manager. What I use to manage passwords.
Go to this link to try RoboForm Free;
if you like it you can upgrade to RoboForm Everywhere version with all the features
With Roboform, you will have one less thing to feel stressed about. (affiliate link)






