This information is current as of the date of original publication or update but may have changed by the time you read this. Do not use this information for diagnosis or treatment purposes. Before making health decisions, discuss with a qualified healthcare professional.
“The Opioid Crisis”
If you follow the news at all, you’ve probably read or heard about the opioid or, more recently, the fentanyl crisis. It was and continues to be an issue in national and local elections, with every candidate claiming they will solve the problem.
The problems with opioids are alternately framed as legislative, criminal, political, economic, immigration, and terrorism issues.
Opioid use is fundamentally a public‑health crisis, not merely a criminal justice problem.
Opioid use disorder, OUD, is a chronic medical condition that can lead to fatal overdose, infectious disease, and long‑term disability. Treating it as a health issue means providing life‑saving care rather than punishment. Options include medications for opioid use disorder, low‑barrier treatment, and widespread naloxone access.
The harms extend far beyond the individual’s health:
- unstable housing and homelessness, which then increase overdose risk and disrupt continuity of care;
- job loss and reduced workforce participation strain families and local economies; and
- parental substance use endangers children, causes early life trauma, and intergenerational instability.
Effective responses require combining treatment with supportive housing, employment services, childcare, and legal and social support so people can stabilize their lives while receiving care.
This recent article, which I am sharing with permission, reviews current statistics on opioid use in the United States and some of the approaches to dealing with the problems that result.
Drop in opioid overdose deaths nears 50% since 2023
by Tim Henderson, Oklahoma Voice
March 23, 2026
Since their peak less than three years ago, opioid overdose deaths dropped nearly by half as of October 2025, according to a Stateline analysis. The drop comes as a shrinking fentanyl supply has made the drug weaker and less deadly and volunteer efforts get more people into treatment.
The weaker fentanyl tracks to a crackdown on materials used to make fentanyl in China around the time U.S. deaths started dropping in 2023. Some experts see it as a welcome, but possibly temporary, break for states in a scourge that boosted crime as people who are using the drugs sometimes fall into homelessness and steal to support fentanyl habits.
The numbers and rates of opioid overdose deaths fell for all races between 2023 and 2026, according to more detailed data from the federal Centers for Disease Control and Prevention analyzed by Stateline. That’s in contrast to an earlier trend from 2019 to 2023, when rates dropped only among white people and rose sharply among Black and Indigenous Americans.
Ohio had the nation’s largest decrease since mid-2023, when the nation’s opioid overdose deaths peaked. Ohio has seen fewer deaths but more risky behavior lately as fentanyl supplies dry up and people turn to substitutes tainted by animal tranquilizers.
Helping Addicted Persons
Ohio is seeing a difference in the bottom line, said Erin Reed, director of RecoveryOhio, the state agency charged with reducing overdose deaths.
“We’re seeing things you would expect — like reductions in emergency department visits and reductions in Medicaid costs, But we’re also seeing a positive impact on violent crime and recidivism, and I think this is really, really encouraging.
At the end of the day, people want to be safe.”
Erin Reed, director of RecoveryOhio
Sarah Beckman, 36, stopped using illicit drugs 11 years ago when she learned she was pregnant with her first child. Now she works through Hamilton County’s Quick Response Team to help Ohio residents who use fentanyl.
When overdoses peaked a few years ago, the team started spending more time talking to people after overdoses.
“We saw overdoses were going up and up, and going out two days a week was not enough. We expanded it to full-time,” Beckman said. “That window is so small. It has to be kind of a perfect storm for an individual to be, like, ‘OK, I’m ready.’”
Even if people aren’t ready for treatment, kindness can help build trust and prevent some of the thefts and arrests that lead to police involvement, as it did for her when she stole to get money for drugs and was charged with resisting arrest, she said.
When you’re in the midst of addiction you need help with everything. For us it’s just meeting people where they are and saying, ‘Hey, are you hungry? Do you have enough clothes?’
You’re showing consistency and empathy, and by doing that you can slowly move someone closer toward accepting overdose prevention materials or hopefully, eventually, treatment.”
Sarah Beckman, recovered drug user
Where Opioid Deaths Decrease or Increase
Nationally, there were 46,066 opioid overdose deaths in the year ending with October, barely more than half the peak of 86,075 in June 2023 and the lowest since April 2017. The numbers, often delayed because of the process of determining overdose deaths, were released this month based on information available March 1 by the federal National Vital Statistics System.
Deaths fell the most in Ohio, West Virginia, Virginia and Florida since June 2023, but increased in Alaska, Arizona and Nevada.
In Ohio, annual deaths fell 63% from about 4,300 in June 2023 to about 1,600 as of October 2025.
As in many other states, deaths in Ohio started falling before 2023, but then dropped more sharply — 34% in that year alone, said Reed.
Arizona and Nevada, however, saw deaths increase since the national peak in 2023. Arizona’s border crossings with Mexico are among the largest fentanyl smuggling points in the country, with fentanyl traffic dominated by the Sinaloa Cartel in Mexico.
One Arizona crossing, the Port of Lukeville, was the site of the largest fentanyl seizure in U.S. Customs and Border Protection history: 4 million fentanyl pills hidden in a trailer brought to the border by a 20-year-old U.S. citizen in July 2024.
The state’s notorious summer heat exacerbates overdose deaths, according to recent research. Arizona is one of three states with more opioid overdose deaths as of October 2025 than at their national peak in 2023, according to a Stateline analysis.
Plentiful supply from the border may help explain continued increases in Arizona, said Will Humble, executive director of the Arizona Public Health Association, a public health workers organization.
Political infighting over how to spend the state government’s share of $1.2 billion in opioid settlement money hasn’t helped, he said. The state attorney general, governor and legislature have gone to court over plans to use some of the money to balance the state budget.
“Many other states are way ahead of Arizona when it comes to distributing the state portion of the opioid settlement dollars,” Humble said. “It could be there are fewer interventions because the state dollars are locked up. There’s this dispute in Arizona over who gets to decide. Many other states are not having this jurisdictional issue.”
On the national stage, opioid overdose deaths fell across demographic groups. Even older Americans, whose overdose death numbers had surged earlier even as they fell for other groups, saw a 25% decline from 2023 to 2025, about half the national decrease, according to the Stateline analysis.
In a sign of a weaker fentanyl supply, the Drug Enforcement Administration said in December that 29% of the pills it seized in fiscal 2025 contained a lethal dose of fentanyl, down from 76% in fiscal 2023.
“These reductions in potency and purity correlate with a decline in synthetic opioid deaths,” the DEA said.
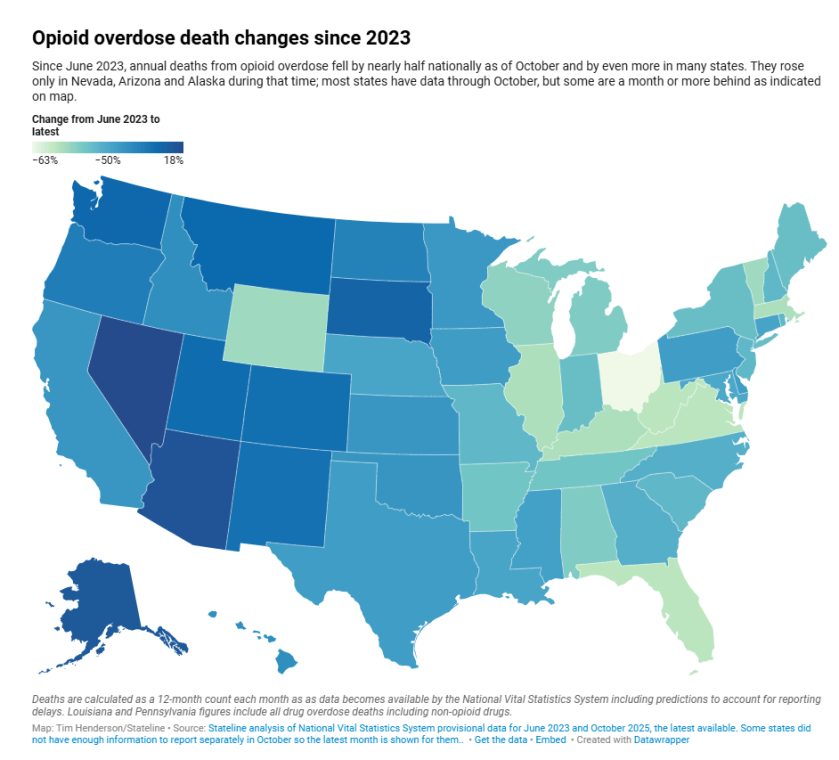
The lighter shades indicate decreased overdose deaths. The darkest shades show increased deaths.
A “Fentanyl Supply Shock”
Keith Humphreys, a health policy professor at Stanford University who testified to the U.S. Senate in 2023 about increases in accidental overdose deaths among older adults, told Stateline that a “fentanyl supply shock” originating in China made fentanyl supplies weaker. That would include fentanyl-tainted cocaine, which had caused many deaths among older Black men, Humphreys said.
“This likely includes some long-term cocaine users who had the bad luck to get cocaine that had fentanyl in it,” Humphreys said in an interview. White women are more likely to overdose on prescription drugs in order to commit suicide, a trend that would be less likely to be affected by fentanyl supply, he added.
Humphreys and a team of other researchers, in a Science magazine report published in January, found a “drought” of fentanyl that could be traced on the social media platform Reddit.
Elevated mentions of a “drought” started in May 2023, nearly the same time as overdoses began to drop, their research found. Also, the Drug Enforcement Administration reported decreasing potency in seized fentanyl and fewer seizures, both indicating a shortage of supply.
“Drug dealers often adapt to supply shortages by lowering purity more than raising prices,” the report stated. The likely reason: China cracked down on source chemicals for making illicit fentanyl. Such “precursor” chemicals typically arrive from China and are processed in Mexico before being smuggled into the U.S. as illicit fentanyl.
“Actions by the government of China that resulted in greater scrutiny of production and export of precursor chemicals, including the removal of online advertisements and several marketplaces,” may have been what caused the drought in fentanyl and thus saved lives, the report concluded.
The DEA concluded that Mexican fentanyl producers were cutting potency because they were having a hard time finding source chemicals from China, the report noted. That makes it likely supply is the biggest reason for the drop in deaths, not enhanced U.S. border searches or other actions such as the Trump administration’s attacks on drug boats off the South American coast. Those boats are typically used to transport cocaine rather than fentanyl.
Data shows a similar drop in overdose deaths in Canada, where fentanyl supplies are usually produced from Chinese chemicals inside the country rather than smuggled in. That’s another reason to suspect that China’s crackdown affected both countries, despite differing policies and law enforcement strategies.
Vigilance Still Needed
In their Science article, Humphreys and the other researchers noted that the recent decline in deaths offers the chance to prepare for future opioid-related problems.
“The incentive to restore the fentanyl trade will persist as long as there is demand for the drug,It may be wise to use the current drought as an opportunity to ramp up the prevention and treatment programs that have evidence of decreasing demand.”
Keith Humphreys, in Science magazine
There have been some more recent upticks in death numbers.
Colorado saw an increase in synthetic opioid overdose deaths starting in late 2024, according to a Common Sense Institute report released this month. The institute is nonpartisan but has ties to the Republican Party, and concluded the state needs stiffer penalties for fentanyl possession and distribution, similar to Texas law. Opioid overdose deaths in Colorado are down 9% since the national peak in 2023, according to the Stateline analysis.
In Ohio, the recent trend among people who use fentanyl is to find pills spiked with an animal tranquilizer that causes severe addiction, said Beckman, of the Hamilton County Quick Response Team. Three recent clients survived overdoses but required emergency treatment, she said.
“We can educate people in the community: ‘Hey, your drugs are not what you thought they were, that’s why you’re experiencing all these weird side effects,’” Beckman said. “These substances are so severe that a traditional detox hasn’t been able to handle them.”
Stateline reporter Tim Henderson can be reached at thenderson@stateline.org.
This story was originally produced by Stateline, which is part of States Newsroom, a nonprofit news network that includes Oklahoma Voice, and is supported by grants and a coalition of donors as a 501c(3) public charity.
Oklahoma Voice is part of States Newsroom, a nonprofit news network supported by grants and a coalition of donors as a 501c(3) public charity. Oklahoma Voice maintains editorial independence. Contact Editor Janelle Stecklein for questions: info@oklahomavoice.com.
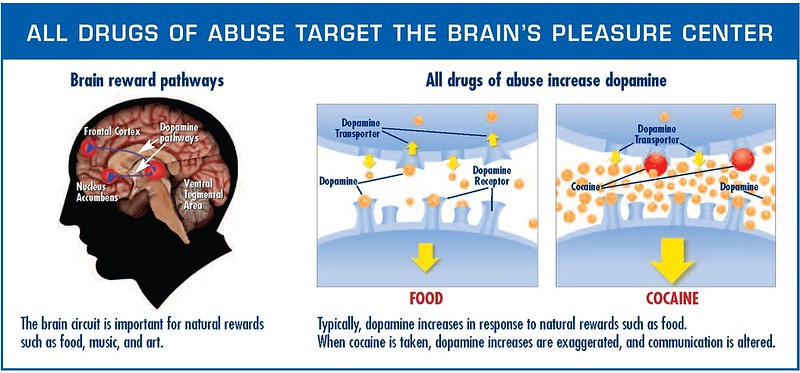
From Treatment to Recovery
Preventing overdose death and finding treatment options are the first steps to recovery. Treatment may save a life and can help people struggling with opioid use disorder get their lives back on track. Treatment can counteract addiction’s powerful effects on the brain and behavior.
The overall goal of treatment is to return people to productive functioning in their family, workplace, and community.
Opioid use disorder treatment can vary depending on the patient’s individual needs, occur in a variety of settings, take many different forms, and last for varying lengths of time.
Evidence-based approaches to treating opioid use disorder include medications and combining medications with behavioral therapy. A recovery plan that includes medication for opioid addiction increases the chance of success.
Medications used in the treatment of opioid use disorder support recovery by normalizing brain chemistry, relieving cravings, and preventing withdrawal symptoms. The evidence for medications to support successful recovery is strong. (source-CDC Overdose Prevention)
SAMHSA’s National Helpline
SAMHSA’s National Helpline is a free, confidential, 24/7, 365-day-a-year treatment referral and information service (in English and Spanish) for individuals and families facing mental and/or substance use disorders.
The cover image was created by AI and approved by me.
Exploring the HEART of Health
I’d love for you to follow this blog and follow me on social media.
I share information and inspiration to help you transform challenges into opportunities for learning and growth.
Add your name to the subscribe box to be notified of new posts by email. Click the link to read the post and browse other content. It’s that simple. No spam.
I enjoy seeing who is new to Watercress Words. When you subscribe, I will visit your blog or website. Thanks and see you next time.
Use this search box for related posts on this blog or other topics of interest to you.
Dr. Aletha
- About Dr. Aletha
- How to Use this Site
- Make Your Life Easier
- Search by Category
- Share the HEART of health
- my Reader Rewards Club
- RoboForm Password Manager