You’re probably used to your doctor’s office using an EMR, electronic medical record (also called EHR, electronic health record) . By now most clinics, private medical offices, hospitals, labs, imaging centers, and other healthcare settings use computers exclusively for everything from scheduling, communication, to documentation and billing. If you are a young adult, you may not even remember a time when medical offices and hospitals used paper records.

Dr. Danielle Ofri, author of several books about healthcare delivery, wrote an astute opinion piece about EMRs for STAT which I encourage you to read. I’m going to review her post adding my own ideas, , with the goal of helping you understand why we doctors, and maybe you, have a love/hate relationship with computers in healthcare; as Dr. Ofri says about electronic health records,
they all have their breathtaking assets and snarling annoyances
Dr. Danielle Ofri
In her piece, Dr. Ofri refers specifically to the use of electronic records in hospitals, but the issues are similar in clinics and other settings.
Breathtaking assets
- more efficient storage of records than paper (taking up less physical space and time for sorting and filing)
- ability to generate reports
- improved hospital efficiency and financial margins (possibly by the ability to analyze data and generate reports)
- able to analyze the health needs of large numbers of patients, called population health, so health systems can plan for and offer needed services more efficiently
- communication- the ability to contact doctors by email, get test results through a portal, schedule appointments online, order med refills, etc.
- legibility and standardization in documentation
Snarling annoyances
- changes the way doctors work and make decisions; current software often does not reflect the way doctors are taught to approach patient diagnosis and treatment
- less efficient retrieval of data than paper (due to larger amounts of data, which may be redundant)
- little evidence yet that use decreases complication rates, or improves patient care in general
- less personal interaction with healthcare professionals when communicating through a portal
- increased time spent documenting on a computer , much of it simple data entry, compared to writing on paper
But the greatest disadvantages attributed to the use of computers in the medical setting, ones far more than “snarling annoyances” are
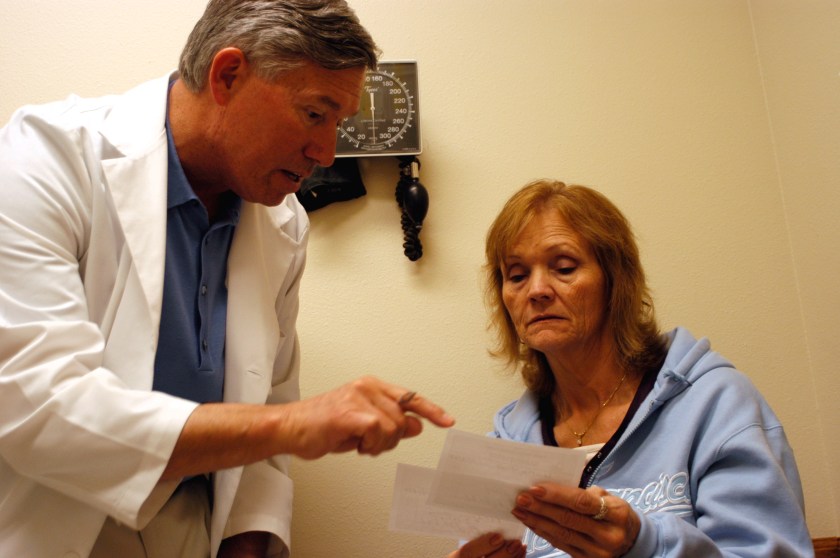
- interference with doctor patient interaction and communication in the office or bedside; both doctor and patient may pay more attention to the computer than to each other
- erosion of staff morale, often due to more time spent on the computer than with the patient, boredom with data entry, and stress of having to learn new systems and updates
- contributing to physician burnout, which can have a negative impact on patient care
Doctors like me, who did not grow up in the computer age, went through the entire medical education experience without touching a computer. For us , the transition to computerization while maintaining a busy schedule of patient visits, was difficult and stressful. The increase in physician burnout has been directly linked to the introduction of electronic medical records.
Boldly going…
As Dr. Ofri points out, the EMR is not going away, and few if any of us want to go back to the old system, as annoying as the new system can be. The annoyances are slowly being worked through and resolved, and the assets are becoming truly helpful.
The younger generation of doctors who have never known a world without computers embrace their use readily. As we senior doctors wind down and eventually retire, we can pat ourselves on the back for being the generation that led the way into this strange new world.
Where you, the patient, fit in
You as a patient have a stake in this endeavor too. As already mentioned, being able to access your records, make appointments, manage payments, and send messages on your computer or mobile device brings efficiency and convenience to a process that formerly was time consuming and cumbersome. I now routinely use my doctor’s office portal for my own medical needs and my patients use my office’s online services . Here’s what you can do to help make EMR use better.
- Use whatever online healthcare resources available to you. The more we all use them, the easier they will be to use, and feedback will help developers make them even more helpful.
- Be patient with your doctors and other healthcare providers as they transition to EMRs, from one to another, or when problems occur. Like any piece of technology, they don’t always work perfectly, and occasionally they don’t work at all.
- Give constructive feedback. A thoughtful critique will help more than irate criticism.
Here is the link to Dr. Ofri’s article-
The EMR has changed the doctor patient relationship into a menage-a-trois

“you have a role and a vested stake in communicating your concerns, questions, and even grievances to the physicians who care for you; that without such information, your physicians cannot provide optimal diagnosis and treatment for you. ”
from my review of Dr. Ofri’s book -at this link
What Patients Say, What Doctors Hear
Danielle Ofri, M.D., is a physician at Bellevue Hospital, a clinical professor of medicine at the New York University School of Medicine, editor-in-chief of the Bellevue Literary Review, and author of the forthcoming book
When We Do Harm: A Doctor Confronts Medical Error

Another physician explores the EMR
MAN’S 4TH BEST HO$PITAL By Samuel Shem
Samuel Shem (pen name of Stephen Bergman, M.D.) is a novelist, playwright, and, for three decades, a member of the Harvard Medical School faculty. His other novels include The House of God, Fine, and Mount Misery .

In this novel about a hospital dominated by computer screens and corrupted by money, an idealistic doctor has one goal: to make medicine humane again. Here is an excerpt-
“Cynical? me? I feed on ideals, on ideal care. I’m so idealistic, to you I sound cynical! And I do not call ’em Electronic Health Records, ’cause they don’t help with health, and may well harm it. With a screen between you and your patient, you get distracted, right? It’s like texting while driving.
So, to remind us of the danger let’s call ’em EMRs, the ‘M’ for “Medical’. “
After a student asks why the computer systems at the VA (Veterans) and the Indian Health Service hospitals, both government agencies, are more user friendly, he goes on to explain,
“Nobody’s makin’ money offa it. So we all gotta get together and unhook care from billing. So nobody makes an obscene profit offa the sick.”
available on Kindle (affiliate link)

exploring the HEART of the health record
I hope you found this discussion enlightening; maybe it answered some questions you had about electronic health records and maybe raised some issues you’d like to know more about. Please contact me with questions and I’ll answer them in a follow up post.
Dr. Aletha
RoboForm Password Manager. What I use to manage passwords.
Go to this link to try RoboForm Free;
if you like it you can upgrade to RoboForm Everywhere version with all the features
With Roboform, you will have one less thing to feel stressed about. (affiliate link)